The API Is Not the Hardest Part
After spending more time working with SATUSEHAT integrations, I slowly realized something important:
The biggest challenge is not the API itself.
Most modern backend engineers can eventually learn:
- REST APIs,
- OAuth flows,
- JSON payloads,
- and HTTP integrations.
Those problems are manageable.
The real difficulty comes from something much larger:
engineer readiness.
Because SATUSEHAT integration is not just about learning one API.
It's about navigating an entire ecosystem of healthcare standards, terminology systems, workflows, and implementation assumptions simultaneously.
And for many developers, this ecosystem is completely unfamiliar.
The Documentation Problem
One of the first things that becomes overwhelming is how fragmented the learning process is.
A developer trying to build SATUSEHAT integration quickly discovers that knowledge is scattered across multiple ecosystems:
- SATUSEHAT implementation guides
- FHIR documentation
- LOINC terminology references
- HL7 specifications
- healthcare workflow concepts
- OAuth and authentication documentation
Nothing exists in one unified developer experience.
Instead, engineers are expected to move back and forth between standards bodies, implementation guides, terminology references, and API documentation just to understand how a single workflow should operate.
And this creates a very different onboarding experience compared to most modern developer platforms.
Healthcare Standards Have a Steep Learning Curve
FHIR itself is already a large ecosystem.
Then developers discover:
- coding systems,
- terminology bindings,
- resource relationships,
- references,
- profiling,
- validation rules,
- and healthcare-specific workflow logic.
At that point, the integration work stops feeling like "API integration."
It starts feeling like entering an entirely different industry.
Because in many ways, it is.
And while large organizations may have interoperability specialists, many hospital IT teams are expected to learn these concepts while simultaneously maintaining existing hospital systems.
The SDK Question
One thing I kept asking myself during implementation was:
Why are hospitals repeatedly rebuilding the same integration layer independently?
A national-scale platform has significantly more:
- engineering resources,
- institutional support,
- and financial capability
than individual hospital IT teams.
Yet most of the implementation burden still happens downstream.
Instead of official SDKs that abstract common integration complexity, developers are primarily given:
- documentation,
- Postman collections,
- and sandbox environments.
Technically, that may be enough to start integrating.
But operationally, it means every institution still needs to solve many of the same engineering problems independently.
The Cost of Repeated Engineering Work
Across hospitals, developers are repeatedly rebuilding similar infrastructure:
- request wrappers
- token lifecycle handling
- FHIR resource validation
- terminology mapping
- retry handling
- integration abstractions
- data transformation layers
Not because these problems are unique.
But because every institution is forced to solve them on its own.
At national scale, this creates an enormous amount of duplicated engineering effort.
Hundreds of teams spending time rebuilding similar foundational layers instead of focusing on improving healthcare systems inside their own institutions.
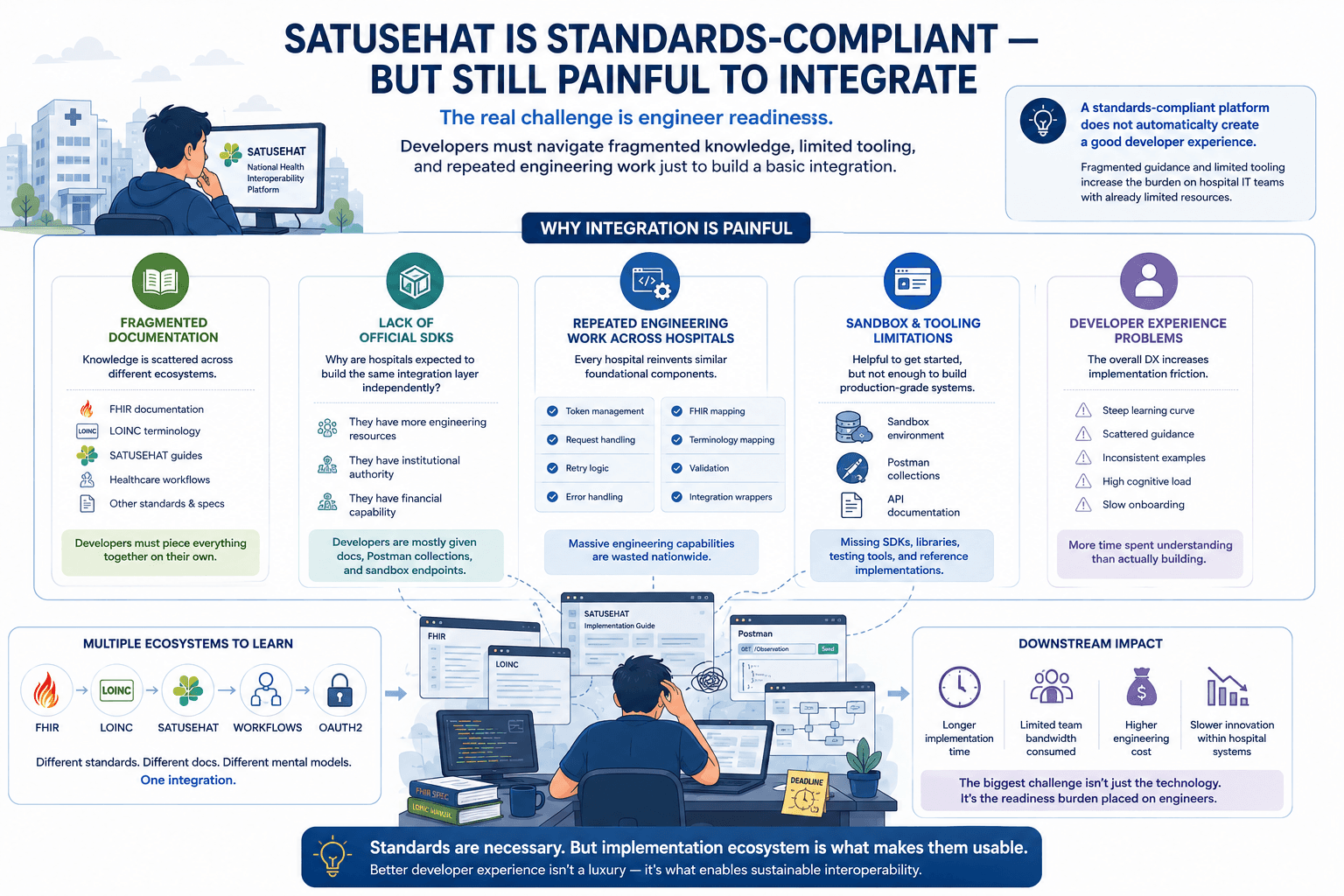
Standards Compliance Is Not Developer Experience
This is probably the biggest thing I learned during the integration process:
A standards-compliant platform does not automatically create a good developer experience.
A system can:
- follow specifications correctly,
- implement international standards,
- and still be difficult to adopt operationally.
Because developer experience is not just about technical correctness.
It's also about:
- onboarding clarity,
- implementation guidance,
- abstraction layers,
- tooling quality,
- and how much cognitive load gets pushed onto engineers.
And in healthcare interoperability, that cognitive load becomes very large very quickly.
Closing Thoughts
I don't think the problem is that healthcare interoperability standards are unnecessary.
Standards absolutely matter.
But implementation ecosystems matter too.
Because every layer of fragmented knowledge, missing tooling, and repeated engineering work increases the readiness burden placed on hospital IT teams.
And when interoperability depends on every institution independently overcoming that burden, implementation difficulty scales far beyond the API itself.
The challenge is no longer just technical integration.
It's whether the ecosystem is realistic for the engineers expected to implement it.