Interoperability Looks Different Under Pressure
In theory, interoperability is supposed to improve healthcare systems.
Better data exchange. Better coordination. Better continuity of care.
And at a high level, those goals make complete sense.
But implementation reality inside hospitals often looks very different from the idealized diagrams shown in presentations and policy discussions.
Because once interoperability becomes tied to compliance deadlines and operational consequences, priorities begin to shift.
The conversation stops being:
"How do we build sustainable interoperability?"
And slowly becomes:
"How do we make sure we pass compliance requirements?"
That difference matters more than people realize.
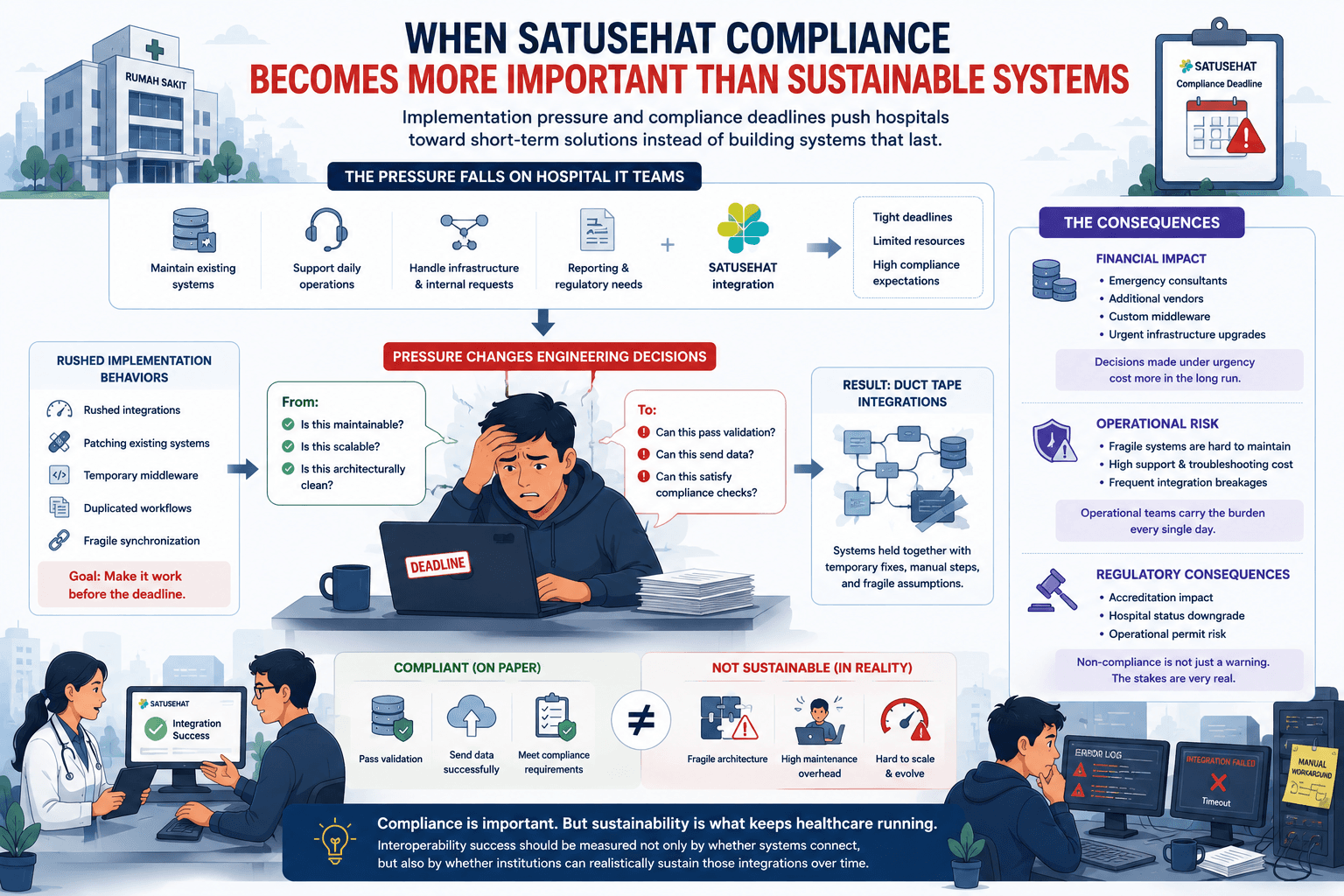
The Pressure Falls on Internal IT Teams
When interoperability mandates arrive, the pressure usually does not land on policy designers or standards committees.
It lands on hospital IT teams.
Teams that are already responsible for:
- maintaining existing systems,
- supporting daily hospital operations,
- handling infrastructure issues,
- responding to internal requests,
- and keeping critical workflows functioning.
Then suddenly they are expected to:
- understand healthcare interoperability standards,
- implement SATUSEHAT integration,
- adapt legacy systems,
- and meet regulatory deadlines,
often with limited manpower and limited interoperability experience.
At that point, the objective changes.
The goal is no longer building elegant architecture.
The goal becomes:
"Make it work before the deadline."
Compliance Pressure Changes Engineering Decisions
This is where many interoperability discussions become disconnected from operational reality.
Because under enough pressure, engineering decisions become survival decisions.
Instead of asking:
- Is this maintainable?
- Is this scalable?
- Is this architecturally clean?
teams start asking:
- Can this pass validation?
- Can this send data?
- Can this satisfy compliance checks?
And honestly, that's understandable.
Hospitals operate under real regulatory consequences.
Failure to comply is not treated as a minor inconvenience.
The stakes can become extremely serious:
- accreditation impact,
- hospital status downgrade,
- or even operational permit risk.
That changes everything.
The Rise of Duct Tape Integrations
Under those conditions, short-term solutions become very tempting.
And sometimes unavoidable.
Hospitals may:
- rush integrations,
- patch existing systems,
- build temporary middleware,
- duplicate workflows,
- or deploy fragile synchronization logic
simply to achieve compliance targets as quickly as possible.
Not because engineers don't care about quality.
But because operational pressure leaves very little room for long-term system design.
The result is what many engineers informally call:
duct tape architecture.
Systems held together by temporary integration layers, manual processes, and fragile assumptions that become increasingly difficult to maintain over time.
The Financial Consequences
Implementation pressure also creates financial pressure.
Hospitals that lack internal interoperability expertise may suddenly need:
- external consultants,
- emergency integration support,
- additional vendors,
- custom middleware,
- or rapid infrastructure upgrades.
And because deadlines are involved, decision-making often happens under urgency instead of long-term planning.
Ironically, this can increase costs significantly.
Not because interoperability itself is inherently wasteful.
But because rushed implementation environments rarely produce efficient engineering outcomes.
Compliance Does Not Automatically Mean Sustainability
This is probably the most important thing I've realized while observing interoperability implementation:
A compliant system is not always a sustainable system.
A hospital may technically:
- pass integration requirements,
- successfully send data,
- and satisfy operational mandates,
while internally relying on fragile workflows that are difficult to maintain long-term.
From the outside, the ecosystem appears connected.
But internally, many teams may still be struggling operationally.
And that distinction matters.
Because interoperability success should not only be measured by:
- whether systems connect,
but also by:
- whether institutions can realistically sustain those integrations over time.
Closing Thoughts
I still believe interoperability is necessary.
National healthcare ecosystems require coordination, standardization, and shared infrastructure.
But implementation pressure has consequences.
When compliance urgency grows faster than institutional capacity, hospitals naturally prioritize immediate operational survival over long-term architectural sustainability.
And honestly, that's not a failure of individual engineers or hospitals.
It's a predictable outcome of systems where implementation burden, regulatory pressure, and engineering readiness become misaligned.
Because in the end, healthcare interoperability is not just about connecting systems.
It's also about whether the institutions expected to implement those systems can realistically sustain them.